
Lessons, Practices, and a Survivor-Centered Playbook
On March 20, 2023, I participated in a panel a decade after the Boston Marathon bombings to examine what worked, what did not, and how communities and leaders can carry forward improvements in emergency preparedness and response. I led Boston's public health preparedness office at the time and want to center the practical actions my team and partners took, the behavioral practices that made the difference, and the specific steps leaders can use now to strengthen readiness for mass-casualty incidents, natural disasters, and complex public health emergencies.
Why this matters: outcomes, survivors, and systems
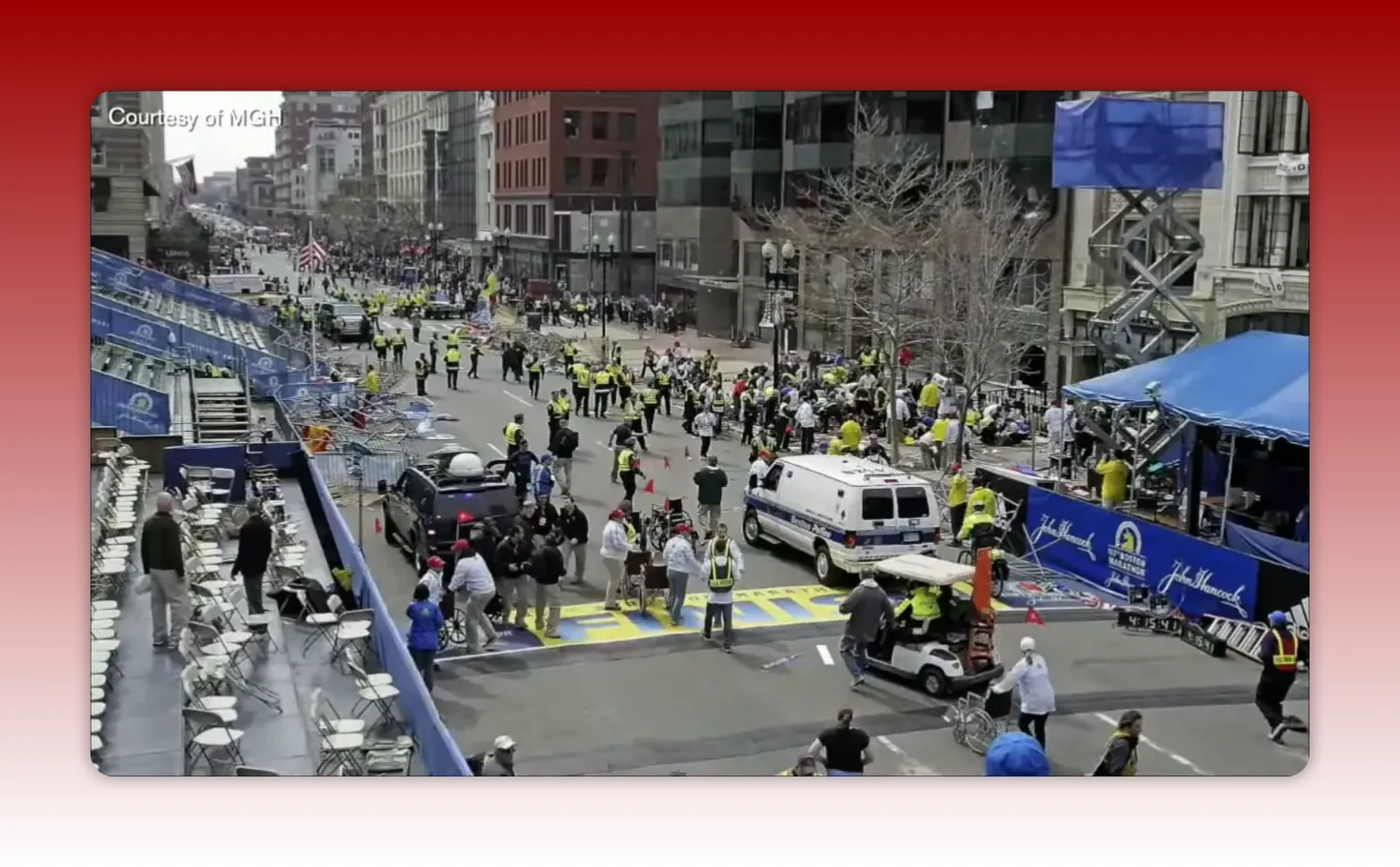
The Boston Marathon response demonstrated that planning, training, and cross-sector coordination can dramatically increase survival after sudden mass-casualty events. Nearly every person who arrived alive at a hospital survived. That outcome was the product of systems and people working together: pre-positioned medical supplies and equipment, practiced triage and transport patterns, rapid patient tracking, and a civic willingness to help.
But superior immediate outcomes are only part of the story. Long-term recovery, survivor support, mental health care for responders, equity in access to help, and sustainable funding are equally important. Preparing for emergencies is therefore both clinical and social. This article explains concrete practices that made the difference and offers checklists that leaders and organizations can implement.
Overview: what I will cover
Core preparedness systems that mattered
How to switch from special-event operations to disaster response
Clinical and logistical lessons (tourniquets, blood, amputation care)
Behavioral framework: swarm leadership in practice
Mental health, survivor support, long-term recovery, and equity
Communications and social media lessons for modern incidents
Actionable leader checklists and training recommendations
What made Boston’s preparedness effective: the core systems
Several institutional elements that existed before April 2013 created the foundation for the rapid, coordinated response. I focus here on systems I worked with directly and how they translated into action.
1) Medical Intelligence Center (MIC)
What it is: A central coordination node linking public health, EMS, hospital incident command, and emergency planners. The MIC aggregates incoming patient data, supply needs, bed availability, and situational reports so that resource allocation is timely.
Why it mattered: The MIC allowed us to track patient flow in real time, identify surges in need (for example, blood or surgical supplies), and coordinate distribution across hospitals instead of overloading one facility.
2) Multi-agency training and a standing special-events posture
Boston treats the Marathon as more than a race: it is an annual, full-scale exercise. Hospitals, EMS, police, transit, public health, and volunteer networks use the event to test communications, triage, reunification, and transport protocols. Repeating full-scale exercises and smaller tabletop drills builds muscle memory and clarifies roles before an incident occurs.
3) Cross-discipline institutional relationships
Trust-based relationships among chiefs, agency directors, and hospital leaders reduce friction in crisis. Years of joint training and formal policy conversations meant people knew who to call, who had authority for what, and which agency would assume responsibilities in different geographies.
Switching modes: from special event to disaster response
One of the most difficult operational moments is the need to shift from a planned-event posture to an incident command structure without losing continuity. The Marathon showed three practical approaches that helped:
1) Predefined role-transition protocols
Define in advance how volunteer and event staff are accounted for and reintegrated into an incident response. This prevents confusion about personnel availability and protects volunteers' safety.
2) Immediate patient-tracking and family reunification
Runners and spectators often arrive at hospitals without personal identification or possessions. Establish a centralized reunification center and digital tracking protocols so family members can be matched to patients quickly and with minimal re-traumatization.
3) Rapid inventory redistribution
Expect atypical clinical needs. After blast injuries, hospitals needed surgical sets, tourniquets, and prosthetic planning. A MIC or similar mechanism should monitor needs and move supplies between facilities without delay.
Clinical lessons that saved lives
Clinical practice and equipment standards are often revised by experience. The Marathon response highlighted three clinical changes that became widely adopted:
Stop the Bleed and tourniquet use
Tourniquets and hemorrhage-control tactics were decisive. Widespread training and placing bleeding-control kits in public venues can turn bystanders into life-saving responders. Programs that teach basic hemorrhage control for civilians and first responders (Stop the Bleed style curricula) should be institutionalized.
Massive transfusion readiness
Large-scale bleeding events require blood management protocols. Pre-coordination with regional blood banks, contingency transfers from neighboring jurisdictions, and emergency donor mobilization plans prevent shortages.
Surgical capacity and limb-salvage planning
When multiple patients require complex vascular and orthopedic surgeries—or amputations—create predefined plans to distribute surgical cases across trauma centers to avoid exceeding any one operating room capacity. That includes quick identification of prosthetic and rehabilitation resources for longer-term care.
Swarm leadership: the behavioral architecture that complements structure
Structure and resources are necessary, but not sufficient. The behavioral dynamics—how leaders act and how people cooperate—were a second, equally powerful determinant of success. We identified five behavioral themes that I witnessed and helped facilitate.
1) Unity of mission
When everyone adopts a single, clear objective—saving lives and minimizing harm—decisions across agencies become aligned. Clear mission statements, communicated and repeated, reduce paralytic debate and enable fast operational choices.
2) Generosity of spirit and action
Generosity means sharing resources, jurisdictional flexibility, and creative problem solving. Examples include assigning National Guard troops to support police searches or allowing unarmed uniformed personnel to perform minimal-security tasks to free sworn officers for other duties.
3) Strong but flexible chains of command
Chains of command must be respected and clear, but also adaptable. People staying "in their lanes" while trusting others to do their jobs reduces duplication, conserves resources, and prevents public confusion.
4) No ego and no public blame
Leaders who downplay personal credit and avoid public finger pointing maintain cohesion. When conflicts arise, resolve them privately so the public sees unity. Emotional self-regulation in leadership is a practice as important as tactical training.
5) Trust-based relationships
Trust is the outcome of years of joint training and shared experience. These relationships allow rapid delegation and acceptance of responsibility across agencies and municipalities. Investing in routine joint activities builds this trust before it is needed most.
Mental health, survivor support, and long-term recovery
Immediate clinical success does not end a disaster's human impact. A responsible response includes mental health care for survivors, witnesses, first responders, and families. It also includes a plan for long-term social and economic recovery.
Mental health support embedded in response
Employee assistance programs and hospital mental health teams are necessary but often overwhelmed. Pre-arrange surge mental health capacity with state or federal mental health response teams and community providers, and embed them into hospital responses to assist clinicians and staff exposed to traumatic injuries.
Family Assistance Center best practices
Set up a secure, survivor-focused family assistance center with a small number of vetted agencies providing coordinated services: victim compensation counseling, legal aid, medical navigation, and social supports. Limit the number of agencies that interact directly with families to avoid repeated retelling of traumatic details.
Long-term recovery planning
Recovery includes rehabilitation, home modification for disabilities, vocational support, and business recovery for affected storefronts. Establish a single fund or one-stop mechanism for distributing financial aid quickly and transparently—delays deepen trauma and impede recovery.
Equity and community-centered response
Not everyone experiences emergencies the same way. Equity considerations must be built into planning:
Include community-based organizations in planning and operations so distribution of help is culturally competent and accessible.
Track who receives services and resources to identify gaps by neighborhood, race, language, or socioeconomic status.
Ensure communication materials are multilingual and accessible to people with disabilities.
We observed that some communities felt left out of the "Boston Strong" narrative. Equal focus on all affected populations is essential to credible and just recovery.
Communications and social media: speed, transparency, and risks
Social platforms are now central to incident information flow. The Marathon response showed the dual nature of social media: a force multiplier for outreach and a vector for rumor and harm.
Principles for modern communications
Be first, be factual, be brief. Quick acknowledgments of issues—even if incomplete—reduce rumor. Use short, verified updates frequently.
Designate trusted channels. Identify and amplify a small number of authoritative accounts and a cadence for updates to reduce noise.
Use social listening actively. Monitor reports from the public to detect emergent concerns and misinformation; respond quickly to correct harmful narratives.
Anticipate crowdsourced investigations’ harm. Encourage community assistance but caution against public naming or shaming of unverified suspects; set guidance for responsible civic participation.
Platforms and APIs change rapidly. Build flexible data collection and verification processes that can adapt to platform evolution.
Actionable checklists: what leaders and organizations should do now
Below are consolidated, practical checklists you can adopt or adapt for your agency, hospital, or community-based organization.
Pre-incident (preparedness)
Institutionalize annual full-scale exercises that include hospitals, EMS, public health, police, transit, and community organizations.
Create or strengthen a Medical Intelligence/Coordination Center that can operate 24/7 in surge mode and has pre-established data feeds from hospitals.
Stock hemorrhage-control kits and tourniquets in public venues and train staff and volunteers in their use.
Establish mutual aid agreements for blood, specialized surgical capacity, and mental health surge teams with neighboring jurisdictions.
Develop family reunification protocols with a pre-identified physical center and digital tracking tools.
Build survivor-centered long-term recovery plans including a one-stop fund distribution plan that can launch immediately.
Invest in relationship-building—regular joint meetings among leaders across agencies and sectors to build trust.
During an incident (response)
Declare a clear, single mission and communicate it repeatedly.
Activate the MIC or equivalent to coordinate patient flow, supply distribution, and hospital capacity.
Open a Family Assistance Center immediately with a small, trained team to handle reunification and direct family communication.
Mobilize hemorrhage-control resources and prioritize training for bystanders and volunteers at the scene.
Use pre-established mutual aid to move supplies and staff where needed, rather than ad-hoc requests that create duplication.
Coordinate public messaging across agencies to present a unified front and reduce public confusion.
Post-incident (recovery)
Deploy mental health surge teams to hospitals, responder groups, and communities; schedule follow-ups for months and years when needed.
Implement a single fund or streamlined compensation process and expedite initial payments for urgent medical and housing needs.
Track equity metrics to ensure all affected communities receive equivalent support.
Conduct transparent after-action reviews and embed lessons into policy and training.
Training and exercises: design tips that produce results
Exercises should be more than compliance. Use these design choices to increase value:
Simulate role switches—practice moving from planned event mode to incident command, including volunteer accounting and reallocation of staff.
Include behavioral objectives in exercises such as demonstrating unity of mission, refusing to play public blame games, and using pre-arranged trust channels.
Run multi-day scripts that include acute response, investigation phases, and longer-term recovery tasks.
Test family reunification and data flows with realistic identification challenges (hands-off approaches for privacy and trauma mitigation).
Involve community organizations and victim advocates in planning and exercising to identify accessibility gaps before an incident.
Common pitfalls and misconceptions
Leaders often assume technical fixes alone will solve response problems. The Marathon experience shows mistaken assumptions can cost time and trust.
Mistake: "If we have the equipment, people will automatically use it correctly." Reality: Training, refreshers, and practical drills are necessary for correct use.
Mistake: "Public messaging should avoid acknowledging uncertainty." Reality: Timely, transparent updates—even when incomplete—reduce rumor and panic.
Mistake: "Volunteer coordination can be improvised." Reality: Volunteers must be accounted for and integrated into response plans to avoid safety risks and confusion.
Mistake: "Mental health care can wait." Reality: Early, embedded mental health support prevents longer-term disability and sustains workforce resilience.
Mistake: "One-size-fits-all recovery programs are equitable." Reality: Recovery must be tailored and tracked to ensure disadvantaged communities receive proportional support.
Resources and recommended readings
For program managers and leaders who want to dive deeper, look for comprehensive after-action reports, evidence-based hemorrhage-control curricula, and multi-agency readiness frameworks. One particularly detailed operational review is the Boston Marathon Bombings Emergency Support Function 8 After Action Report, which documents health and medical sector response and recovery lessons and is publicly available through municipal or state emergency management repositories.
Frequently asked questions
What is swarm leadership and why is it useful in emergencies?
Swarm leadership describes a set of behavioral practices that complement command-and-control structures. It emphasizes a shared mission, generosity across agencies, disciplined chains of command, suppression of ego and public blame, and trust-based relationships. These behaviors speed coordination and reduce friction during rapidly evolving crises.
How do you set up a Family Assistance Center quickly and effectively?
Identify a single, secure location ahead of time; pre-agree on a small roster of qualified partner agencies (victim assistance, legal, mental health, medical navigation); assign trained case managers to reduce repetitive retelling; set communication schedules with law enforcement for investigation updates; and transition to virtual services when appropriate for long-term follow-up.
What immediate actions reduce mortality after a blast or mass-trauma incident?
Rapid hemorrhage control (tourniquets, wound packing), efficient triage, even distribution of patients across trauma centers, and prompt access to blood and surgical services are the top clinical drivers of survival.
How should agencies manage social media during a crisis?
Establish authoritative channels, provide short frequent updates, use social listening to identify and counter misinformation, avoid naming unverified suspects, and coordinate messaging across agencies to present a unified information posture.
How can smaller jurisdictions apply these lessons if they lack resources?
Smaller jurisdictions can focus on relationship building, shared training with neighboring jurisdictions, mutual aid agreements for critical supplies, embedding hemorrhage-control training in community programs, and establishing a simple family reunification protocol using existing community centers and digital tools.
Final reflections and an invitation to act
Participating in the panel a decade later reminded me that preparedness is both an organizational discipline and a moral commitment. Systems like a Medical Intelligence Center, annual full-scale exercises, and Stop the Bleed training saved lives. But the quieter investments—building trust among agencies, committing to survivor-centered recovery, embedding mental health supports, and focusing on equity—are equally important and often under-recognized.
Leaders can take practical steps today: run a multi-agency exercise that includes family reunification, commit to a hemorrhage-control program for public events, map long-term recovery resources and a single funding pathway, and foster trust through regular cross-sector convenings. These are high-value, achievable actions that make a measurable difference when the next crisis arrives.
For practitioners and policymakers who want a starting point, convene an interagency working group this quarter to review: your MIC capability, mass transfusion plans, family reunification procedures, and survivor recovery pathways. Prioritize the actions that will change lives in the first 72 hours and sustain support for months and years after.
Acknowledgement
These recommendations reflect years of collaborative work across public health, EMS, hospitals, law enforcement, community organizations, and survivors. Preparedness is a team sport—one that requires routine practice, humility, and a focus on care for people most affected.
This article was created based on the video The Boston Marathon bombings a decade later: An inside look at lessons learned.


